News
We Should Be Humble International Press Conference
We Should Be Humble When Facing the Dignity of Life?? International Press Conference
We just held an international press conferece on Aug.12, which was about the sad case of misdiagnosis of Ms.Serena Wu's son, Pinghsien, who passed away last year at the young age of 21. Serena investigated into Pinghsien's death and found that his disease is in fact Carnitine Deficiency, instead of NAGS deficiency. For her, it is already hard to accept the her son's death, let alone the cruel truth that all the effort spent on fighting against her son's disease turned out to be so wrong.
However, she decides to get out of the emotinal tangles and view the whole issue from a larger scope. Her only wish is to save more patients who might have the same condition as Pinghsien's illness by telling the story and raise patients' and medical professional's alertness. She hopes that we will all learn the lesson from the loss of her beloved son's life. We share this sad case with you and hope that this would teach more people the importance of correct diagnosis, second opinion and research on complications of rare diseases and hopefully we can avoid the same tragedy from happening again.
----------------------------------------------------------------------------------------
We should be humble when facing the dignity of life<<< Because we can't live twice!
Gene Tells the Truth
A Hasty Diagnosis Led to a Cruel Truth that Should Never Have Happened
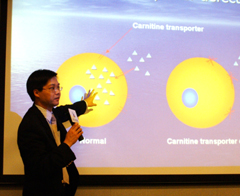
In a nitrogen freezer located in the corner of Dr. Chin-Yuan Lin's lab, some of Pinghsien's skin tissue still waits to be brought back to life. Dr. Lin has thawed out part of Pinghsien's skin tissue and resurrected it for testing. Skin tissue doesn't speak but it can still tell us the mysterious mistake and grief of the past 16 years.
("Can Pinghsien Live Twice?", Serena Wu,)
On Aug. 14, 2005, a sudden cardiac failure struck a young man at the age of 21 and took his life while he sat at his reading desk. It was too sudden for him to call for help and get to the hospital. His shocked father could only watch his beloved son dying. The young man is Pinghsien Wu.
Conflict and Sadness motivated her to seek the truth
Revealing the truth starts with a frank and responsible doctor at National Taiwan University Hospital
After Pinghsien's death, filled with struggle and sadness, Serena had doubts about her son's death. She knew very well that her son’s disease had been under control and that things shouldn't have ended this way. She was determined to find out the truth. Finally, after 10 months of hard work, she found out that Pinghsien's disease was in fact Primary Carnitine Deficiency and Secondary NAGS Shortage. Furthermore, carnitine supplement, which has been considered as supplemental, turns out to be the essential medication that was
sustaining Pinghsien's life. Pinghsien didn't take carnitine during Serena's trip to the U.S. and this led to his death. Serena said, “We were never informed that it was a matter of life and death for Pinghsien to take the carnitine.” Misdiagnosis led to counteractive treatment and medical advice and eventually caused a cruel and irreversible tragedy.
Two sad ifs, Three heartfelt appeals
Facing the mystery of life with a humble heart
If Pinghsien's American doctors hadn't made an over-confident diagnosis and followed it up with a nine-page paper, would I have had the chance to keep investigating the true cause of Pinghsien's illness? Would I have known where to go, whom to ask, and what to look for?
If Pinghsien's Taiwanese doctors had challenged the so-called authoritative diagnosis and investigated Pinghsien's severe carnitine deficiency, would the truth have been revealed in time to avert the tragedy?
(Serena Wu, "Can Pinghsien Live Twice?”)
After Pinghsien's death, Serena had thousands of questions and had phoned the U.S. doctor who gave the diagnosis in 1990, asking "Why do patients of urea recycle disorder need to take carnitine? Is Secondary Carnitine Shortage the cause of heart disorder such as ventricular hypertrophy? Are they related? Dr. Vockley just replied that some patients with metabolic disorders have to take supplemental carnitine to correct a Carnitine Shortage. But he didn't think Carnitine Shortage was related to Pinghsien's heart problems. Even after Serena confirmed Pinghsien's real disease and notified him, so far Dr. Vockley hasn't given any formal response...
For Dr. Hwu, chairman of Medical Genetics Department, NTUH, who took care of Pinghsien, Pinghsien's sudden death is a regrettable and disappointing result. He said, “People in Taiwan tend to feel that the grass is greener on the other side of the fence and they usually try their best to seek medication and treatment abroad. The U.S., because of its advanced medical science, has become for many people the ideal place to receive treatment. However, there are a great variety of rare diseases and each of them is complicated. In recent years, medical science in Taiwan has improved a lot and become more advanced, so people and physicians should have more confidence in Taiwan medical science. When we find something suspicious, we should all check carefully and look for truth to prevent the same tragedy from happening again.”
We wish to make three appeals based on the sad case of Pinghsien. We hope these appeals will prevent the same tragedy from happening to other families:
Appeal 1. Since it is very difficult to diagnose a rare disease, diagnosis and confirmation require great care.
The 21st century is an era when people enjoy advanced technology and medical science. However, when confronting the great mysteries of life, what we actually know is very little. We should always be humble when facing the dignity of life.
According to the survey conducted by Global Views Monthly in 2003, 15.5% of people above the age of 18 believe that they have experienced misdiagnosis (June, 2006 Global Magazine Monthly, Jia-Huei Hsu). Research released in 2005 by FDA and NIH also indicated that up to 36% of tuberculosis cases in the study were misdiagnosed. It took on average up to 4.5 months before the misdiagnoses were corrected. Even then, it was found that in fact 4% of the patients had cancer rather than tuberculosis. In these cases, medical resources were wasted, and so was time that could have been spent on the correct treatment. Anguish and despair is usually the reaction after finding such news.
When a common disease such as tuberculosis is so easily misdiagnosed, we can't help worrying that the situation for rare disease patients is even worse. Rare disease patients often have to go through many hurdles before they receive the correct diagnosis. They are often initially diagnosed with more common diseases. For instance, patients of motor neuron disease often have to see many different specialists such as orthopaedics and ENT because of their various symptoms. They are frequently diagnosed with myasthenia gravis or nerve compression. Furthermore, Multiple Sclerosis patients' symptoms vary every time the disease strikes them and they are often diagnosed with brain tumors, mood disorder, or optic neuritis, delaying treatment or physical therapy.
Rare disease patients often go through several misdiagnoses and treatments, and they often wander between different hospital departments. The time spent seeking medical advice and diagnosis often lead to delays in treatment, to missing the early stage of disease when treatment is most effective, and even to death. Thus, we appeal strenuously for a more organized, precise and painstaking rare disease diagnosis system to be established as soon as possible, in order to improve the quality of medical treatment, honor the rights of rare disease sufferers, and respect the dignity of life. Prof. Yuan-Tsong Chen, Director of Institute of Biomedical Sciences, Academia Sinica and chairman of the board of TFRD described the way the process should work when he said “If the gene sequence mutation cannot be found, doctors should not give the diagnosis. Mistakes happen. When they do, doctors
should have the courage to admit it.”
Appeal 2: It is important for patients and physicians to seek a second opinion on rare disease diagnosis and treatment.
Human beings make mistakes! We know that no doctors hope to make mistakes. We know that diagnosis and treatment are far more difficult for rare diseases than for common ones. An ideal medical environment would be one in which doctors attentively inquire into patients' conditions, speculating on the cause of disease carefully and formulating treatment to attack the root of the disease. In the medical system, patients almost always lack medical knowledge. What patients know is far more less than what doctors know. And therefore patients should seek medical advice from many doctors, and actively exchange opinions with doctors, provide detailed symptom descriptions, disease histories and other relevant information in order to help doctors give correct diagnoses. Doctors should also actively help patients get second opinions. This is a great challenge but it is also to respect life. We hope that the domestic medical environment will gradually become more open so that patients and their families, who already suffer great anguish facing the diseases, would receive full consultation and assistance.
Furthermore, even though the quality and quantity of research on rare diseases have improved a lot, there is still much to do. Strengthening international exchange with overseas medical research centers is another important issue.
Appeal 3. Research on complications of rare diseases is lacking. Teamwork is the key to save life.
Rare diseases are not only hard to diagnose and treat. They also involve many potentially fatal complications. Complications make fighting against rare diseases a great challenge. For instance, it is easy for patients of Williams Syndrome and Prader-Willi Syndrome to get diabetes mellitus type II, so their blood sugar needs to be monitored. Patients of Duchenne Muscular Dystrophy will have complications such as cardiac failure and pneumonia. Patients of Hereditary Epidermolysis Bullosa often have skin infections that sometimes result in squamous cell carcinoma. These complications are threats to patients' lives. There are patients who find the real cause of their diseases when treating their complications. (Please see attachment 3.)
Take Bojing, who also has carnitine deficiency, for example: he received the correct diagnosis because of a consultation held before his heart surgery. Now that he has received correct treatment, he is doing well (Please see attachment 4). Bojing has a different life from Pinghsien because he received the correct diagnosis and treatment. How can
Pinghsien's family accept this result?
It is sad to see these stories happening repeatedly while research on complications of rare diseases is still insufficient. Only through exchange between and integration of foreign and domestic medical teams can this problem be solved. We hope this problem can be resolved as early as possible to prevent more similar mistakes and tragedies from happening.
Medical personnel have people's trust, and respect. They must strive to fulfill the responsibility that rests on their shoulders: this is their mission; this is what they must dedicate themselves to.
After losing her beloved son, Serena has turned from grief to understanding: instead of holding a grudge and blaming the doctors or seeking compensation through legal action, she has formulated several appeals in the hope that both medical personnel and patients learn the universal value: respecting life. She hopes we can all face life and death with great caution and composure. Rare disease patients bear the brunt of the risk of evolution and inheritance on behalf of humanity, dedicating their precious lives. We must give our most precious gifts to humanity, just as Pinghsien gave his life!
If Pinghsien's American doctors hadn't made an over-confident diagnosis and followed it up with a nine-page paper, would I have had the chance to keep investigating the true cause of Pinghsien's illness? Would I have known where to go, whom to ask, and what to look for?
If Pinghsien's Taiwanese doctors had challenged the so-called authoritative diagnosis and investigated Pinghsien's severe carnitine deficiency, would the truth have been revealed in time to avert the tragedy?
What we want to emphasize is, medical personnel who serve rare disease patients have people's trust and respect. This increases their responsibility to their patients. It requires great discretion and perseverance to fulfill their job responsibilities. This is hard work that brings along great pressure. However, life is precious and a single thought or decision may make a crucial difference. Medical personnel should repay people's trust and respect with an attitude of responsibility and humility. And patients will pay them back with endless gratitude and respect.




500 Join International Rare Disease Day Event
Feb.01, 2026

FOXG1 Syndrome Patient Association Established
Jan.11, 2026

Annual Gathering For Volunteers From All Regions
Dec.22, 2025

APARDO 10th Anniversary Conference
Dec.01, 2025
AADC Deficiency Patient Gathering
Nov.30, 2025

Spreading Love Through Music
Nov.29, 2025

The 23rd Scholarship and Grant Awards Ceremony
Nov.15, 2025

Caregivers’ Healing Workshop
Oct.27, 2025